The Great Medicaid Transition: Thriving in the evolving Medicaid reimbursement era
As Medicaid shifts to PDPM, SNFs must act now. Learn how knowledge, communication, and technology are separating reimbursement leaders from laggards.

The winds of change are sweeping across the Medicaid landscape — and for those of us working in skilled nursing facilities, standing still is no longer an option.
The shift from RUG-IV and other reimbursement methodologies to the Patient Driven Payment Model for Medicaid reimbursement is transforming how care is documented, measured and ultimately reimbursed. While some states are already knee-deep in the transition, others are cautiously wading in or haven’t even dipped a toe.
But regardless of where your state stands, there’s one truth we can’t ignore: Proactive management is the new mandate.
Medicaid State of the States: A patchwork of progress
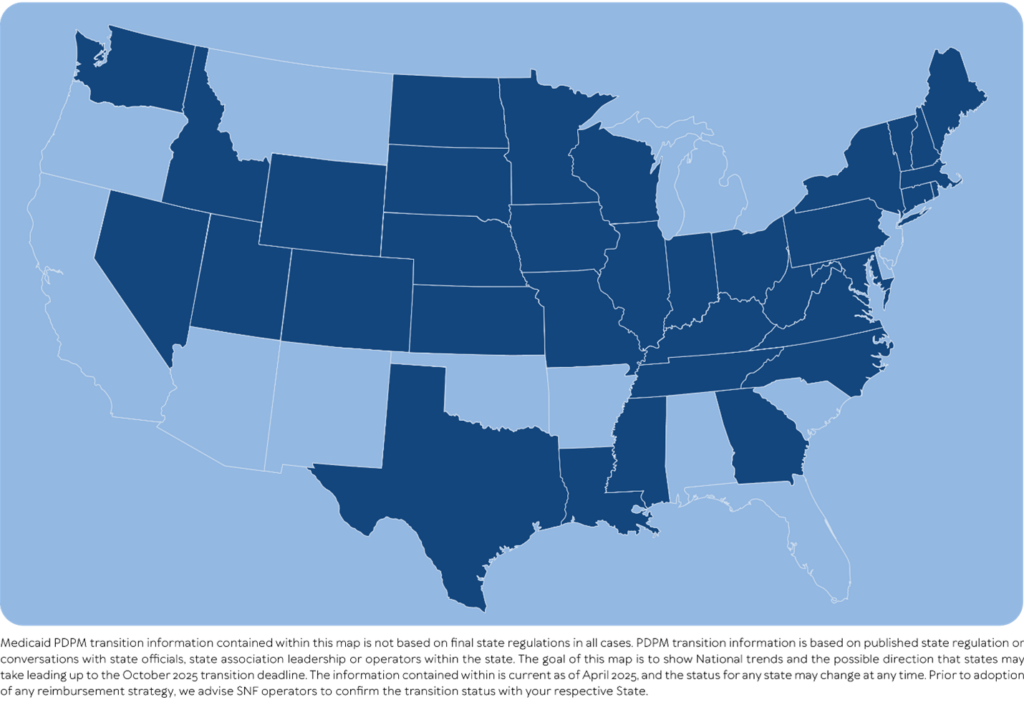
Medicaid’s adoption of PDPM is anything but uniform. Figure 1 identifies states that utilize any form of MDS-based CMI system.
Figure 1
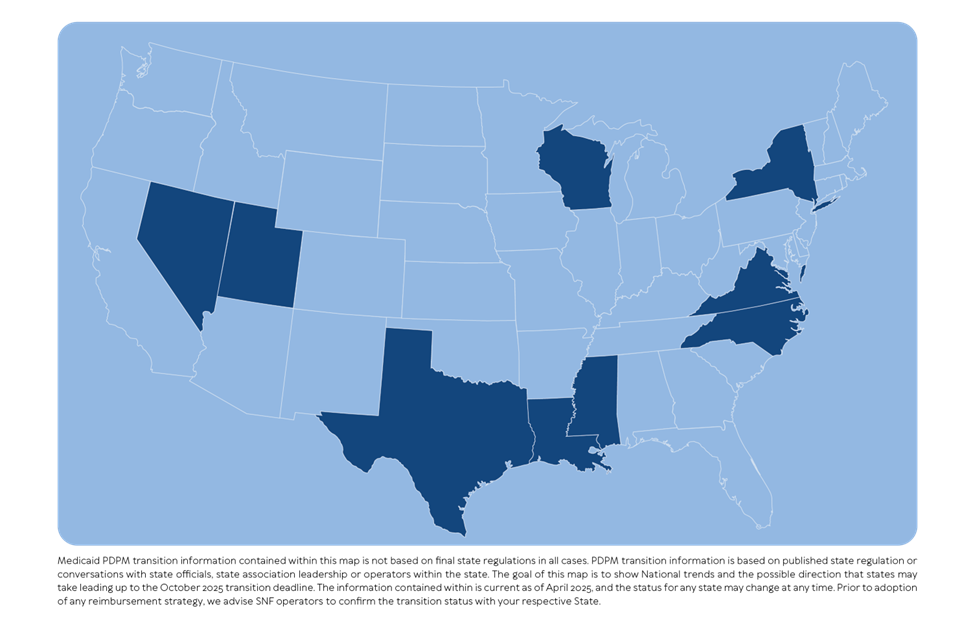
However, even with those states that do adopt a PDPM CMI-based strategy, there is tremendous variability. For example, Figure 2 shows states that have already adopted or will likely adopt the PDPM Nursing component.
Figure 2

And Figure 3 shows states that have already adopted or will likely adopt more than one PDPM component, such as the nursing and NTA categories.
Figure 3
This inconsistency creates a complex environment for multi-state operators. But it also offers an opportunity — if we have access to proper education, technology and act early.
While the transition is theoretically budget-neutral (what’s given to one facility is taken from another), the early adopters of education, communication and technology are capturing greater reimbursement now. Eventually, the rest will catch up — but that early momentum can be a game changer.
So, what separates the leaders from the laggards? According to CMI-Connect, four key factors determine a state’s speed of transition and provider success:
- Previously existing reimbursement system
- Type of state transition (cold turkey vs. gradual)
- State’s adherence to RAI manual
- State-specific auditor aggressiveness
SNFs need to position themselves ahead of the curve — by mastering the new system before it masters them.
From studying providers in states that have already transitioned to PDPM Medicaid reimbursement, three pillars for success were distilled: Knowledge, Communication, Technology.
1. Knowledge
PDPM brings a host of intricacies that can’t be mastered passively. Misunderstandings lead to missed opportunities. Everyone — from MDS coordinators to rehab staff — must understand the “why” and “how” behind the new system. And remember: Some states have “gone beyond” how the RAI guides key items completion, adding their own spin.
2. Communication
Transitioning from a RUG or other reimbursement methodology to PDPM isn’t a solitary endeavor. It requires robust collaboration among the entire interdisciplinary team. Social workers, nurses, therapists and physicians must align to ensure data is accurate, timely and compliant. Simply put, the more you communicate, the more accurate acuity is identified. Opportunities are lost when assumptions are made about who should interview the residents.
3. Technology
With acuity driving reimbursement, the tools we use to identify and track clinical complexity have become mission critical. Traditionally, we have relied on “what’s on the MDS assessment” and kept our fingers crossed that all acuity was captured. Yet acuity isn’t always captured on the MDS but is elsewhere in the medical record. Here is where “upstream technology” coupled with thoughtful strategy and human insight is a proven game changer.
Figure 4 demonstrates how early adopters in one state of “upstream” technology, who embrace educational and interdisciplinary communication, are “winning” the Medicaid CMI transition.
Figure 4
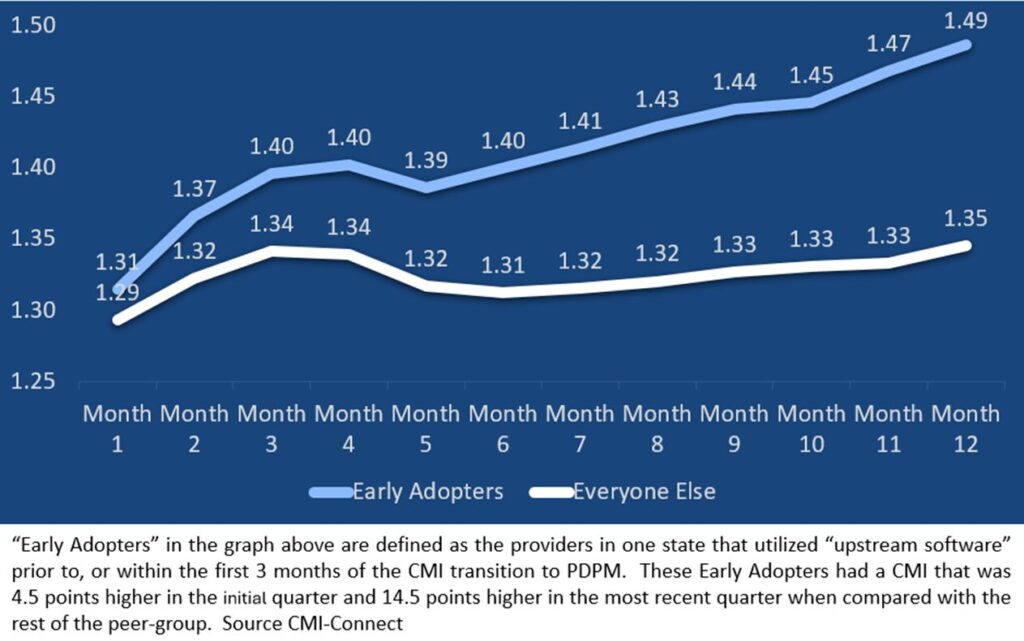
While each state transition to PDPM will vary, we expect almost all states to follow a similar pattern of case-mix “creep.” Preliminary data from early adopters in other states that have more recently converted to PDPM show a similar early trend in performance.
Act now, reap later. The Medicaid PDPM transition is a journey — one that rewards preparation and punishes complacency.
SNFs that embrace education, prioritize communication and invest in smart technology are not only better positioned financially, but they are also providing better, more accurate care, all within an environment of compliance.
Steven Littlehale is a gerontological clinical nurse specialist and chief innovation officer at Zimmet Healthcare Services Group.
The opinions expressed in McKnight’s Long-Term Care News guest submissions are the author’s and are not necessarily those of McKnight’s Long-Term Care News or its editors.