The due diligence dialect: Is Five-Star simply noise?
CMS Five-Star ratings now drive lending, payer access, and capital decisions but experts warn the system's flaws make it a risky sole measure of facility quality.

In long-term care, data drives dollars. Investors, lenders, operators and policymakers increasingly turn to metrics to guide billion-dollar decisions — but what if we’re chasing the wrong signals?
For over 15 years, the Centers for Medicare & Medicaid Services’ Five-Star Quality Rating System has served as the industry’s unofficial “gold standard” for evaluating nursing home performance. A high star rating suggests operational excellence. A low one? Financial risk.
But as the system evolves and its influence expands, we must ask a critical question: Does Five-Star actually tell us what we think it does, or are we mistaking correlation for causation?
The origin story: Built for consumers, repurposed by everyone else
When CMS launched Five-Star in 2008, its intent was simple: Empower consumers to make informed choices about selecting a nursing home. But over time, the system took on a life of its own. Lenders, investors, payers, attorneys and policymakers began treating the star ratings as a shorthand for operational health and risk exposure:
- Lenders and REITs use them to guide underwriting and portfolio risk.
- Commercial payers and MCOs use them to gatekeep network participation.
- Attorneys leverage them in plaintiff and defense strategies.
- Media and policymakers amplify them, shaping reputational risk and political pressure.
Five-Star became much more than a consumer tool — and CMS itself played a central role in making that happen.
How CMS made Five-Star unavoidable
While Five-Star wasn’t designed to influence capital allocation or network access, CMS decisions hardwired ratings into financial viability. Two areas stand out:
1. Alternative Payment Models (APMs). Many CMS-led APMs, including the new TEAM model, require participating nursing homes to maintain at least a 3-star rating. For operators, this means:
- Falling below three stars can exclude facilities from potentially lucrative contracts.
- Lower-rated facilities lose access to three-day stay waivers, which allow direct SNF admissions without a qualifying hospital stay.
- A star rating below the minimum could jeopardize preferred hospital and payer partnerships.
In other words, a facility’s stars now determine its seat at the table.
2. HUD 232 financing and the “Express Lane” advantage. The HUD Section 232 loan program provides financing for the purchase, refinance, or rehabilitation of SNFs — and within it, the “Express Lane” process has become a critical advantage for borrowers. Here’s where Five-Star comes in:
- Facilities with 4- or 5-star ratings often qualify for streamlined underwriting under the Express Lane pathway.
- Express Lane applications enjoy faster approvals, fewer documentation requirements, and more favorable debt terms.
- Facilities with 2-star ratings or below, however, face enhanced scrutiny, longer processing timelines, and sometimes denial of expedited access altogether.
For lenders and investors, this creates direct capital consequences tied to ratings. For operators, dropping below three stars isn’t just reputational — it can limit refinancing options, restrict liquidity and increase borrowing costs.
By linking eligibility and pricing advantages to Five-Star thresholds, HUD has effectively amplified CMS’s policy signal, turning the star rating into a gatekeeper for access to affordable capital.
The July 2025 shift: A system on overdrive
In July 2025, CMS made some quiet but powerful changes:
- Health Inspection scoring now relies on two annual surveys instead of three, making ratings more sensitive to recent citations.
- Complaint deficiencies are now frontloaded — the most recent year counts the most.
- Facilities in the bottom 20% of each state automatically receive 1 star for the Health Inspection domain.
- CMS continues to recalibrate benchmarks monthly, increasing volatility.
For operators, this means one bad survey can rapidly sink a facility’s rating. For lenders, it means heightened portfolio risk overnight.
Where stars meet strategy
Here’s why all of this matters:
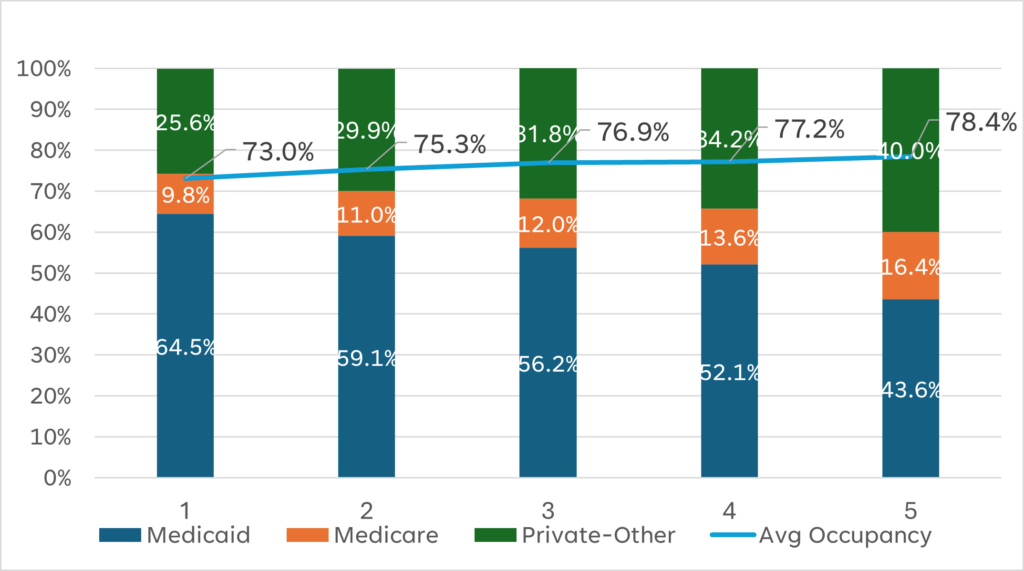
- Higher Five-Star ratings correlate strongly with higher occupancy and a preferred payer mix. This is a national finding but holds up in many local environments. (See Chart A.)
- Most APMs, including those tied to three-day stay waivers, require 3 stars or more.
- Lower ratings can increase insurance premiums, limit hospital partnerships and create litigation exposure.
- Through HUD’s Express Lane program, a facility’s stars now influence its balance sheet.
Chart A: Five-Star Is Correlated with Higher Occupancy and “Preferred Payer Mix”
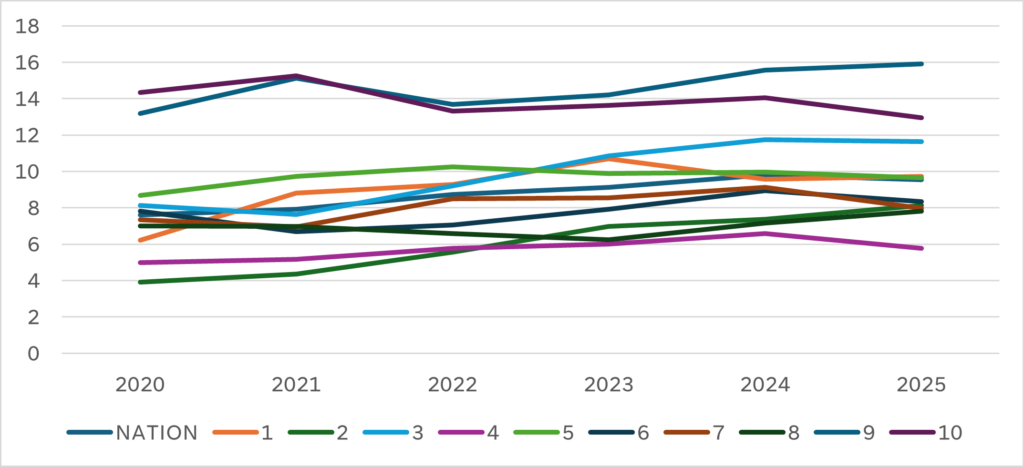
But here’s the catch: Five-Star is principally driven by survey performance, and survey practices vary widely by state. A facility delivering exceptional care in one state might rate lower than a peer delivering average care in another — not because of outcomes, but because of ZIP code.
In Chart B, we see how much survey performance differs by CMS survey district.
Chart B: Average Number of Deficiencies by CMS Region by Year
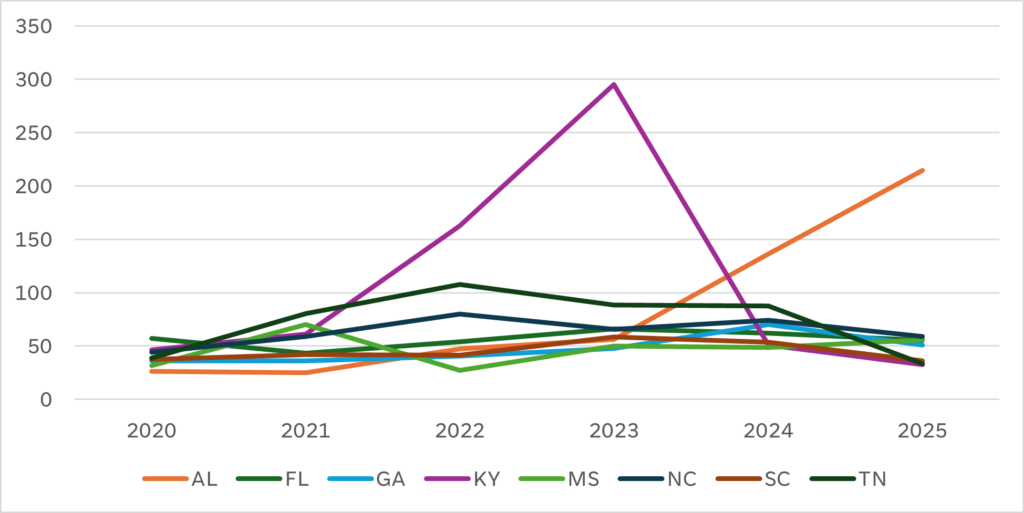
This inconsistency appears not only within a CMS region, but within each state in a region, as we can see in Chart C.
Chart C: Average Total Health Score by State Within CMS Region 4
The call to action: Look beyond the stars
Overreliance on Five-Star creates a self-reinforcing cycle:
- Operators chase stars instead of focusing on holistic quality improvement.
- Lenders tie valuations and financing terms to potentially lagging indicators — CMS ratings refresh only quarterly.
- Facilities struggling with low-star status face reduced capital access, which can limit improvements and perpetuate low ratings.
This loop widens the gap between perception and reality, and in many cases, capital chases stars instead of substance.
Jay Gormley, who heads the advisory division at Zimmet Healthcare, makes another important point: “Five Star is a moving target. CMS keeps changing the formula, so you are not tracking operator performance over time, you are tracking shifting rules.”
But here’s the important nuance: Five-Star isn’t always the best predictor of facility risk. When we analyze all nursing homes terminated from Medicare and Medicaid since 2022, the majority fell within the 1-star group for Overall, Health Inspection, and Staffing. However, some terminated facilities held ratings in these domains as high as 5 stars. (See Table 1.)
Table 1: Distribution of Star Ratings Among Terminated Facilities
Overall RatingHealth InspectionStaffingQM114011816352251582060355674384454665668561496370Blank26193243
This shows us two critical truths:
- High ratings do not grant immunity from operational, regulatory or financial failure.
- Low ratings aren’t destiny either. They signal risk, but they don’t tell the whole story.
When lenders or policymakers rely too heavily on Five-Star, they risk missing hidden vulnerabilities and mispricing actual risk exposure.
Gormley adds: “Quality belongs in underwriting, but Five-Star was built for consumers, not credit committees. It should inform the conversation, not dictate the outcome.”
Tying it together
CMS didn’t intend for Five-Star to define lending strategies, payer relationships or legal exposure. But through its own policies, it ensured exactly that.
The opportunity for our industry isn’t to abandon the stars; it’s to see beyond them.
Data-informed diligence requires context, nuance and balance. Our decisions — and the quality of care we ultimately deliver — depend on it.
Steven Littlehale is a gerontological clinical nurse specialist and chief innovation officer at Zimmet Healthcare Services Group.
The opinions expressed in McKnight’s Long-Term Care News guest submissions are the author’s and are not necessarily those of McKnight’s Long-Term Care News or its editors.
Have a column idea? See our submission guidelines here.